In What Two Ways Can Brain Injuries Occur?
Original Editor - Wendy Walker and Anna Ziemer
Lead Editors - Wendy Walker, Naomi O'Reilly, Kim Jackson, Rachael Lowe, Vidya Acharya, Lucinda hampton, Kalyani Yajnanarayan, George Prudden, Uchechukwu Chukwuemeka, Shaimaa Eldib, Nicole Hills, Lauren Lopez, Mande Jooste, Tony Lowe, WikiSysop, Simisola Ajeyalemi and Karen Wilson
Introduction [edit | edit source]
Acquired brain injury or head injury are broad terms describing an array of injuries that occur to the scalp, skull, brain, and underlying tissue and blood vessels in the head. Acquired encephalon injury does not include damage to the brain resulting from neurodegenerative disorders like Multiple Sclerosis (MS) or Parkinson'south Affliction. Caused encephalon injuries are broadly classified into; traumatic brain injury derived from an external source and non-traumatic brain injury derived from either an internal or external source.
| Traumatic Brain Injury | Not-Traumatic Brain Injury |
|---|---|
| Falls | Stroke e.k. Haemorrhage, Clot |
| Assaults | Infectious Disease e.g. Meningitis, Encephalitis |
| Motor Vehicle Accidents | Seizure |
| Sport / Recreation Injury | Electric Shock |
| Abusive Head Trauma e.1000 Shaken Baby Syndrome | Tumours |
| Gunshot Wounds | Toxic Exposure |
| Workplace Injury | Metabolic Disorders |
| Kid Abuse | Neurotoxic Poisoning eastward.g. carbon monoxide, lead exposure |
| Domestic Violence | Lack of Oxygen eastward.m. drowning, choking, hypoxic & anoxic injury |
| War machine Actions eg. Blast Injury | Drug Overdose |
Traumatic Brain Injury [edit | edit source]
Traumatic Encephalon Injury (TBI) is "an alteration in brain part, or other show of brain pathology, acquired by an external forcefulness".[1] It occurs when an external force impacts the encephalon, and often is caused past a blow, bump, jolt or penetrating wound to the head. However, not all blows or jolts to the head cause traumatic brain injury, some just crusade bony damage to the skull, without subsequent injury to the brain. Mild traumatic brain injury is at present more commonly referred to as Concussion.
Traumatic encephalon injury does non always result in obvious motor impairment. Other hidden symptoms related to cognition and behaviour can too occur with traumatic encephalon injury. The fact that the population living with traumatic encephalon injury are largely invisible and are not outspoken about their needs plus widespread misunderstanding of the impact of related conditions, has earned the traumatic encephalon injury the name the "silent epidemic". [two]
Various healthcare service-related factors can influence the touch of traumatic brain injury on individuals and social club. These include implementation of algorithm-based best practices in emergency and intensive intendance medicine, implementation of a systematic approach to neurorehabilitation, improved admission to related services and adequate related funding. Where these issues are non addressed, people living with a traumatic encephalon injury tin be prevented from capitalising on the nigh valuable time for rehabilitative treatment which results in significantly increased care costs. Longer-term related unemployability and loss of income affect both traumatic encephalon injury survivors and family members providing intendance. These problems atomic number 82 to an underestimated social cost of traumatic brain injury.
[3]
Causes [edit | edit source]
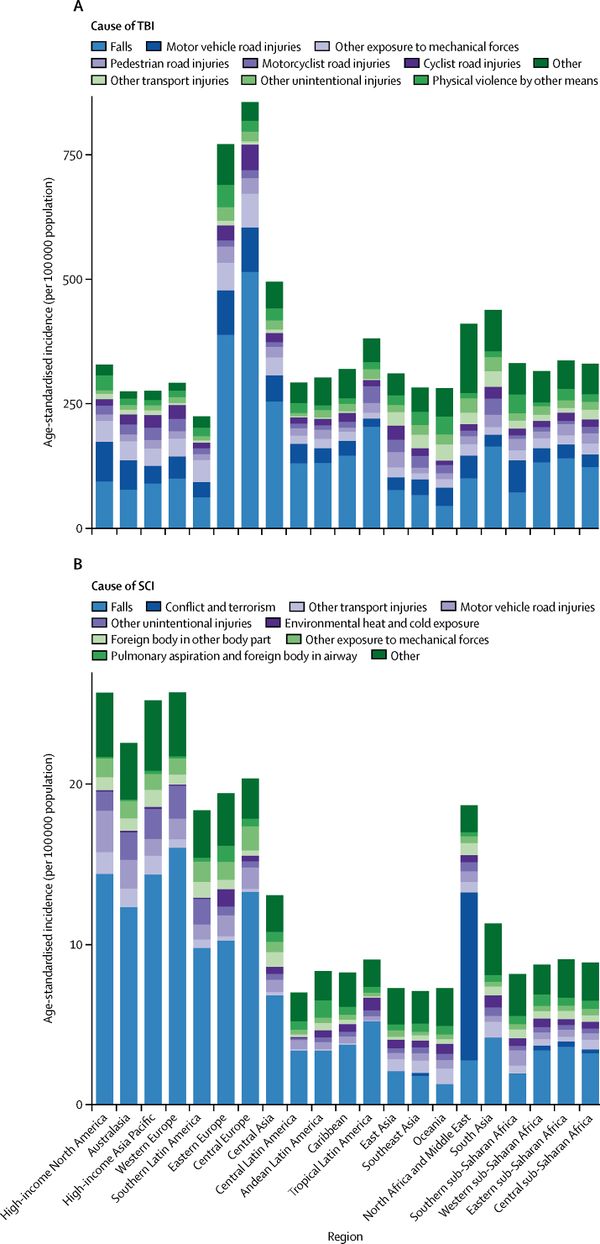
The ii virtually common causes of traumatic brain injury are Falls and road traffic accidents (RTA), which includes vehicle collisions, pedestrians being hit by a vehicle, vehicle-cyclist and car-motorcyclist collisions also every bit wheel and motorcycle crashes which practise not involve some other vehicle. Until recently, road traffic accidents were the primary cause of traumatic brain injury, but an international study published in 2022 reported that "falls have now surpassed route traffic incidents as the leading crusade of this injury". [four]
Traumatic brain injury in sport has go more than recognised with clearly emerging long-term consequences. Many professionals have become involved in developing evidence related to the complexity of symptoms, the impact of the repetitive nature on brain health and long-term prognosis of sport-related concussion. Evidence for sports-specific assessment and handling also as the role of sport in encephalon degenerative diseases are emerging and this is promoting steps to increase the safety of those participating in sports similar rugby, football, battle, horse riding, and racing, American football, or ice hockey. A systematic review carried to find whether the head guards protect against injuries to boxers indicates that concussions and other head injuries are present in battle with or without head guards. A headguard is effective at protecting confronting facial cuts and skull fractures, and a strategy to protect boxers might be to introduce regulations that lower the frequency and strength of blows to the head by incorporating technology into head guards will help understand the type and size of strength sustained past boxers, however, further studies on boxing, headguards, and caput injury prevention are needed.[v]
Global conflicts have exposed the military and civilian participants to new types and severities of injuries, but likewise led to the evolution of improved subacute care and life-saving and neurosurgical procedures,[six] which have also benefited civil healthcare services.
Incidence [edit | edit source]
Traumatic brain injury has been a public health problem for many years and will remain a major source of decease and severe disability in the future. According to the World Health Arrangement by 2022 traumatic encephalon injury volition surpass many diseases as the major cause of death and inability. We are currently observing an increasing number of survivors of traumatic brain injuries due to advances in emergency medicine and intensive care and also due to decreasing fatalities equally a result of safety and preventative measures such as decreased speed limits and the use of helmets and protective equipment. Traumatic brain injury continues to be a disquisitional wellness and socioeconomic problem worldwide beyond low and loftier-income countries due to its life-long consequences and every bit it can affect people at any age. Socioeconomic change in low and middle-income countries due to urbanisation and mechanisation also drives an increase in traumatic brain injury in these regions.
One study found that TBI was "a major cause of decease and disability on the United States, contributing to well-nigh 30% of all injury deaths". [7] A 2010 report looked at information from several nations and reported that "each twelvemonth 235,000 Americans are hospitalised for non-fatal TBI, ane.1 1000000 are treated in emergency departments, and 50,000 dies. A report from Victoria, Australia of traumatic brain injury numbers from 2006-2014 found a decline in the incidence of motor vehicle related astringent traumatic brain injury, suggesting that road injury prevention measures accept been effective, but targeted measures for reducing the incidence of major head injuries from falls should be explored as in the over 65 age bracket these are on the rising. [8] The Northern Finland nativity cohort constitute that three.8% of the population had experienced at least 1 hospitalisation due to traumatic encephalon injury by 35 years of age. The Christchurch, New Zealand nascence accomplice found that by 25 years of historic period 31.6% of the population had experienced at least 1 traumatic brain injury, requiring medical attention including hospitalisation, emergency department, or physician office. An estimated 43.three% of Americans accept residual disability one year after a traumatic brain injury, with the nigh recent estimate of the prevalence of Usa civilian residents living with disability following hospitalisation with traumatic brain injury is 3.ii meg". [9]
We are witnessing a change in traumatic encephalon injury distribution for age groups with children and older people being the highest risk populations; and gender with males beingness the most at risk between ten and 20 years old and females betwixt lxx and eighty [2]. There is also a change in the mechanisms contributing to injury with falls increasingly contributing to traumatic brain injury and blast-related injury beingness the most common mechanism of battlefield sustained traumatic brain injury.
The incidence amongst children and adolescents creates new challenges in the field of traumatic brain injury with often-overlooked symptoms such as behavioural change or educational difficulties and vulnerability to criminalisation.
Access to emergency and neurosurgical services influences bloodshed and recovery outcomes after traumatic brain injury across all earth regions. In lower-income countries, this admission is limited and results in higher numbers of severe disability post -raumatic encephalon injury.
Mechanism of Injury [edit | edit source]
Airtight Head Injury [edit | edit source]
- Often occurs as a result of RTA, or a blow to the caput, or a autumn where the head strikes the floor or another difficult surface.
- In closed head injury, the skull is non penetrated, just it is oftentimes fractured.
- Generally, there is both focal and diffuse axonal damage.
Open Caput Injury [edit | edit source]
- This is caused by a penetrating wound, eg. by a weapon or from a bullet.
- In these cases, the skull is penetrated.
- The brain injury is usually largely focal axonal harm.
Deceleration Injury [edit | edit source]
- This frequently occurs in RTA, when rapid deceleration occurs as the skull meets a stationary object, causing the brain to move inside the skull.
- Mechanical brain injury occurs due to axonal shearing, contusion and brain oedema.
Coup-Contracoup Injury [edit | edit source]
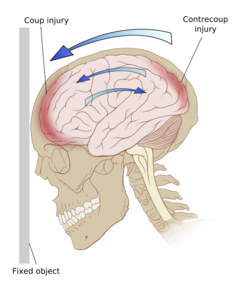
Coup Injury [edit | edit source]
This occurs below the point of touch may exist associated with a skull fracture at the site of impact
Contracoup Injury [edit | edit source]
This occurs when the impact is sufficient to cause the brain to move within the skull; the brain moves in the opposite direction, and hits the opposite side of the skull, causing bruising.
Coup-Contracoup Injury [edit | edit source]
This is a frequent occurrence where opposite poles of the brain endure injury.
Classification [edit | edit source]
At that place are various determinants utilised to classify traumatic brain injury. The clinical presentation and prognosis depend on the individual nature of the injury with unlike types of traumatic brain injury oftentimes coexisting. The nomenclature is of import for acute direction, treatment and prognosis equally well as neurorehabilitation requirements. Classifications may be based on:
- pathoanatomic ie. what damage has occurred and where in the brain;
- injury severity, typically using the Glasgow Coma Calibration every bit the measure where a score of 8 or less is defined equally severe traumatic encephalon injury; or
- past the physical machinery causing the injury, which can be categorised equally contact or "impact" loading when the caput is struck or strikes an object, every bit opposed to non-contact or "inertial" loading, which is when the brain moves within the skull.
Clinical Presentation [edit | edit source]
The presentation depends on the areas of the encephalon which have been damaged. Spasticity is one of the early signs of traumatic brain injury which frequently develops inside a week post-injury. Symptoms include hypertonicity and spasm of the affected muscles and an increase in deep tendon reflexes. The severity of spasticity can range from mild stiffness of the muscles to astringent and ofttimes painful muscle spasms.
Signs and Symptoms [edit | edit source]
Traumatic brain injury tin can have wide-ranging physical, cerebral, psychological and physiological effects occurring immediately or after a flow of fourth dimension has elapsed. The symptoms might differ depending on the severity of the traumatic brain injury, but some are not specific to the blazon of injury.
| Physical Symptoms | Sensory Symptoms | Cerebral Symptoms |
|---|---|---|
| With or without loss of consciousness. If loss of consciousness: a few seconds to a few minutes | ||
| Headache | Blurred Vision | Land of beingness dazed, confused or disoriented |
| Nausea or Vomiting | Ringing in the Ears | Memory or concentration deficits |
| Fatigue or Drowsiness | Bad taste in the mouth or changes in the ability to smell | Mood changes or mood swings |
| Problems with speech | Sensitivity to calorie-free or sound | Irritability |
| Difficulty sleeping or sleeping more than unremarkably | Feeling depressed or anxious | |
| Dizziness or loss of residual | Fatiguability | |
| Physical Symptoms | Sensory Symptoms | Cognitive Symptoms |
|---|---|---|
| Loss of consciousness from several minutes to hours or days | ||
| Persistent headache or headache that worsens | Blurred vision | Coma and other disorders of consciousness |
| Repeated airsickness or nausea | Double vision | Profound defoliation |
| Convulsions or seizures | Ringing in the ears | Irritability |
| Dilation of i or both pupils of the optics | Bad gustation in the mouth or changes in the ability to smell | Agitation, combativeness or other unusual behaviour |
| Articulate fluid or blood draining from the olfactory organ or ears | Sensitivity to light or sound | Distressing or depressed mood |
| Sudden swelling or bruises backside the ears or around eyes | Fatiguability | |
| Disability to awaken from sleep | ||
| Weakness or numbness | ||
| Loss of coordination or residuum | ||
| Irregular animate | ||
| Difficulty speaking | ||
Diagnostic Procedures [edit | edit source]
Post-astute traumatic brain injury, all patients are encouraged to undergo an urgent neurological exam in addition to a surgical examination.[10] Magnetic Resonance Imaging (MRI) and Computerised Tomography (CT) scanning are frequently used in lodge to image the brain. CT scanning is indicated in the very early stages of postal service-injury. A CT scan can show potential fractures and can detail haemorrhages and haematomas in the encephalon, equally well as contusions and swelling. An MRI is ofttimes used once the patient is medically stable to requite a more than detailed view of their brain tissue. The EFNS (European Federation of Neurological Societies) guidelines provide a footing for the use of CT scans based on clinical signs and symptoms (run across below).
| Classification | Characteristics | Referral for CT? |
|---|---|---|
| Mild |
| No |
| Category 1 |
| No |
| Category 2 |
| Yes |
| Category iii |
| Yeah |
| Moderate |
| Yes |
| Severe |
| Yeah |
| Critical |
| Yep |
| Glasgow Coma Scale (GCS), Canadian CT in Head Injury Patients Prediction Dominion (Fleck Rule) | ||
Medical Direction [edit | edit source]
The aims of initial emergency and early medical direction are to limit the development of secondary brain damage while providing the best conditions for recovery from whatsoever reversible damage that has already occurred. This involves establishing and maintaining a clear airway with adequate oxygenation and replacement fluids to ensure adept peripheral circulation with adequate blood volume.
Surgical Interventions [edit | edit source]
Emergency surgery is often required to decompress the injured brain and minimise harm:
- Surgery to remove the haematoma and thus reduce pressure on encephalon tissue.
- Removal of part of the skull in order to save pressure.
- Surgical repair of severe skull fractures, and/or removal of skull fragments from brain tissue.
- Insertion of intracranial pressure (ICP) Monitoring Device.[eleven]
Medical Interventions [edit | edit source]
Medication may also be used to limit secondary damage to the encephalon:
- Coma-inducing medication may be given, as a brain in blackout requires far less oxygen. This is therapeutic where oxygen and nutrient supply to the brain is restricted by compressed claret vessels and increased cerebral pressure.
- Diuretics, given intravenously, can exist used to reduce the amount of fluid in soft tissues and thus assistance reduce pressure on the brain.
- Anti-epileptic medication is often provided in the early stages to avert any boosted brain damage, which may exist caused if a seizure were to occur.[xi]
Physiotherapy Management [edit | edit source]
Just as two people are not exactly alike, no 2 brain injuries are exactly alike. Therefore, the approach to neurological rehabilitation and physiotherapy after traumatic brain injury should observe neuroplasticity, motor learning, and motor command principles too as taking a patient-centred approach with individual interest in goals setting and choice of treatment procedures.
- Initial treatment during the acute phase focuses on promoting respiratory health and prevention of secondary adaptive changes to the musculoskeletal organisation.
- Subacute physiotherapy management focuses on the provision of an appropriate surround to assist functional recovery and on the assisted practise of meaningful tasks, relevant to the ability of the individual, using a full range of treatment modalities.
- Postacute physiotherapy management focuses on reversing secondary adaptive changes and improving specific motor skills with a focus on functional goals for the day to day activities and is dependent on skilled sensorimotor assessment and a collaborative approach with other team members, the individual, and family. This stage tin include inpatient, outpatient, and customs-based settings and for some individuals may require lifelong access to services including planned reviews.[11]
Summary [edit | edit source]
With the complexity of the traumatic brain injury and its wide-ranging consequences, no single medical speciality is sufficient to address all areas of management. In traumatic brain injury direction, the role of the multidisciplinary team is invaluable with the physiotherapist/physical therapist office at its heart from acute to chronic stages.
The increasing recognition of the impact of traumatic brain injury on the private, the family and society is resulting in developments in prevention, service design, legislation and funding. Developments in neuro-protective and neuro-restorative treatments and therapeutic approaches increase neuro-plastic change at cell and network levels. Access to more precise diagnostics is enabling more effective treatment choices. The expertise of specialist medical and rehabilitation centres is becoming more widely shared and implemented. We are living in truly heady times when more than e'er can be done for traumatic encephalon injury survivors.
Resources [edit | edit source]
BrainLine - An American multimedia website providing information and resources almost treating and living with TBI; information technology includes a series of webcasts, written online resource and an electronic newsletter. Information technology has a version in Spanish too.
Model Systems Knowledge Translation Centre (MSKTS) - The Model Systems Knowledge Translation Heart works closely with researchers in the sixteen Traumatic Brain Injury Model Systems to develop resources for people living with traumatic brain injuries and their supporters. These evidence-based materials are available in a variety of formats such equally printable PDF documents, videos, and slideshows.
Headway - A UK charity for TBI which has a comprehensive website, with information on the different aspects of TBI and its rehabilitation. It has a number of useful written resources for patients on the website, including ones on Encephalon Injury and Epilepsy, Loss of Sense of taste and Odor later on Brain Injury and Balance Problems and Dizziness subsequently Encephalon Injury
References [edit | edit source]
- ↑ Menon DK, Schwab One thousand, Wright DW, Maas AI. Demographics and Clinical Cess Working Group of the International and Interagency Initiative toward Common Data Elements for Research on Traumatic Brain Injury and Psychological Wellness. Position statement: definition of traumatic encephalon injury. Archives of Physical Medicine and Rehabilitation. 2010;91(eleven):1637-forty. doi: 10.1016/j.apmr.2010.05.017.
- ↑ 2.0 2.1 Peeters Westward, van den Brande R, Polinder S, Brazinova A, Ewout West, Steyerberg EW, et al. Epidemiology of traumatic encephalon injury in Europe. Acta Neurochirurgica. 2015;157:1683–1696. DOI 10.1007/s00701-015-2512-7
- ↑ Shepard Centre. Understanding Traumatic Brain Injury. Available from: https://youtu.be/9Wl4-nNOGJ0[terminal accessed 30/08/19]
- ↑ Roozenbeek B, Andrew IR, Menon DK. Changing patterns in the epidemiology of traumatic encephalon injury. Nature Reviews Neurology. 2013; 9(4): 231-236
- ↑ Tjønndal A, Haudenhuyse R, de Geus B, Buyse L. Concussions, cuts and cracked bones: A systematic literature review on protective headgear and head injury prevention in Olympic boxing. European periodical of sport science. 2022 Feb xvi:ane-three.
- ↑ Bakery MS. Casualties of the Global War on Terror and their futurity touch on on health intendance and society: a looming public health crisis. Military Medicine. 2022 April;179(4):348-55. doi: 10.7205/MILMED-D-13-00471.
- ↑ Traumatic brain injury in the United states of america: emergency section visits, hospitalizations, and deaths. Faul M, Xu 50, Wald MM, Coronado VG. Atlanta (GA): Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; 2010
- ↑ Medical journal of Australia. Available from: Trends in severe traumatic encephalon injury in Victoria, 2006–2014 (accessed 15 May 2019)
- ↑ Corrigan JD, Selassie AW, Orman JA. The Epidemiology of Traumatic Brain Injury. The Journal Caput Trauma Rehabilitation. 2010;25(2):72-lxxx. doi: x.1097/HTR.0b013e3181ccc8b4.
- ↑ ten.0 ten.1 Vos PE, Alekseenko Y, Battistin L, Ehler E, Gerstenbrand F, Muresanu DF, et al. Balmy traumatic brain injury. European Periodical of Neurology. 2012; nineteen(2): 191-198.
- ↑ xi.0 11.1 11.2 Stokes K, Stack Due east, editors. Physical Management for Neurological Conditions Eastward-Book. Third Edition. Elsevier Health Sciences; 2022 Apr nineteen.
- ↑ Brain Line. Living with a Traumatic Brain Injury. Available from: https://youtu.exist/dyqGys9Htbo[terminal accessed 30/08/xix]
- ↑ TEDx Talks. Follow the patient | Ben Clench | TEDxBrighton. Available from: https://youtu.be/2f1ueKZ8Rxc[final accessed 30/08/19]
jeffersoncatenthe.blogspot.com
Source: https://www.physio-pedia.com/Traumatic_Brain_Injury
0 Response to "In What Two Ways Can Brain Injuries Occur?"
Postar um comentário